The Nonbinary Child
“Man is when short hair and rude in public” say progressives


Fresh from inventing and medicalising the “transgender child”, it seems that doctors are ready to move on to the “nonbinary child”.
We have already seen mad papers suggesting those with a nonbinary identity might want to take, and stay on, puberty blockers1 and now we have a new paper on “nonbinary youth” authored by two paediatric endocrinologists at Seattle Children’s Hospital2 .

Gone, apparently, are the days in which the primary job of endocrinologists is to protect the endocrine systems of their patients.
Now we are in the age of lucrative experimentation.
The paper claims that up to 9% of the general youth population is nonbinary.
The source of this number comes from Spain but given it is being used, here, in an American context, 9% of American youth would work out to be around six and a half million minors.
The authors admit the study showing such a high rate of nonbinary identity, in the general population, may have had a selection bias but they still lead with that figure so I consider that number to be the potential pool of patients they hope to be looking at.
If you look at the table they provide of self-reported nonbinary identity among young people, in various different countries and various samples, the number fluctuates from the more modest 1% to the extraordinary 53.4%.

Imagine how much money these doctors would make medicalising so many young people for life. Note, as well that in the USA sample of patients the age range is 4-17. A four year old who doesn’t sufficiently adhere to the stereotypes pushed on either sex is now, somehow, pathological.
Meanwhile, the staggering 53.4% figure is from a UK sample and in that sample those with a “nonbinary” identity scored higher in anxiety and depression, and lower in self esteem and social support, than those with “binary gender identities”.
So this is a very vulnerable group that medicine now stands to exploit.
The authors talk about the “barriers” to “healthcare” that these young people are experiencing. The obvious fact that what the authors propose to do to these young people is not healthcare, by any sane definition, glides right over their heads like a series of summertime clouds.
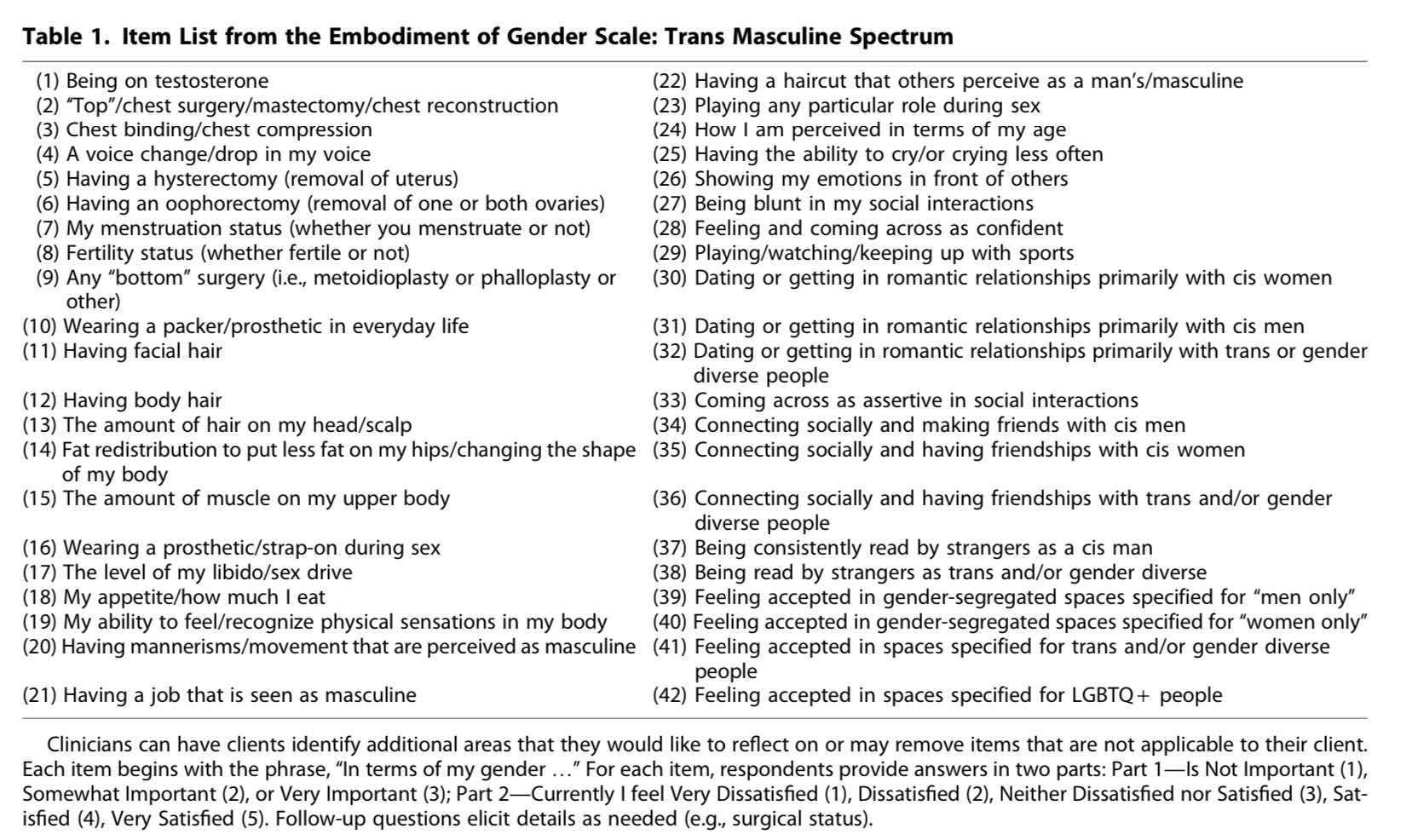
The authors want clinicians to change their language for this group of young people. Terms like “masculinising” and “feminising” (so binary! So last year!) should be dispensed with in favour of terms like “gender embodiment” and asking questions about specific body parts and functions using the Gender Embodiment Scale.
What a grand name for such a lot of codswallop.
It was at this point of reading that I stopped thinking I was going to make this into a quick Twitter thread and opened a Google doc because all of us will want to look at this scale, right? We will want to know the kind of deep science this involves.
The scale itself was developed by others3 and was made for “trans masculine” patients I.e women and girls who identify as men and boys. Or, in the logic of gender identity ideology more towards the male direction. It is interesting to me that our paediatric endocrinologists, who are busily engaged in the denial of the immutable reality of biological sex, nonetheless recognise this scale can be easily used for their patients, too. That is, of course, because their patients are largely female as well.
The language of “uterus haver” and “bleeder” and “bodies with vaginas” that we have long seen promulgated by trans activists, and medical bodies, carves us into parts and functions. The Gender Embodiment Scale seems to treat patients much the same way. These young people are not whole beings who can be understood as such; they are a set of disparate parts that may, or may not, fit an individual’s ideal. These doctors want patients to focus on the aspects of themselves they don’t like so medicine can offer to ‘fix’ them.
For the scale, a set of numbered statements is provided to the patient and they then have to indicate whether it’s “not important”, “somewhat important” or “very important” to them.
So, for example (1) is “being on testosterone”. Then the patient has to say how currently satisfied they are, from very dissatisfied to very satisfied, about each number. A young person who longs to be on testosterone, and isn’t, might say it’s “very important” to be on it, and they are “currently very dissatisfied” because they aren’t.
Is it really coincidental that this kind of ‘survey’ reads like a consumer service review? The bodies of these young people have been made into a product and doctors, with scalpels and prescription pads in hand, aim to offer a bespoke service to amend their earthly ‘flaws’.
Some of the things these young patients will be asked to rate the importance of, and their satisfaction with, are (10) ‘wearing a packer’, (5) ‘having a hysterectomy’, (17) ‘the level of my libido/sex drive’, (20) ‘having mannerisms that are perceived as masculine’, (22) ‘having a haircut that others perceive as a man’s/masculine’, (23) ‘playing a particular role during sex’ and (27) ‘being blunt in my social interactions’.
(“Man is when short hair and rude in public” say progressives).
Also I’m not sure paediatricians of any stripe should be discussing what role their charges take in sex. Quite the red flag if most of them are taking any.
When it comes to adults, I wonder what particular roles are actually supposed to be taken in sex, according to such regressive minds. Active participant is a role open to both sexes now. Women don’t have to lie back, and think of North Derbyshire, anymore.
The Gender Embodiment Scale even has (21) ‘having a job that is seen as masculine’. Are we talking accountant (women bad at maths!) or lumberjack (men good with axe!)?
It’s all a masterclass in the reification of stereotypes. It seems destined to make (mainly) female patients obsess about their bodies further and audit every aspect of themselves and their behaviour. Up to and including (18) ‘my appetite/how much I eat’.
We know there is a higher rate of eating disorders in females who claim a gender identity4 , so I’m not sure what kind of consequence there might be if doctors get them to focus further on how much they eat and then potentially help reframe a dysfunctional relationship to food as “gender affirming”.
I don’t grasp how appetite is relevant to manly feelings under their own rules, either. Unless you’re aiming to eat five dozen eggs a day, like Gaston, food is food and merely fuel for your body. It isn’t gendered. I doubt the implication, here, is that women and girls who identify as men, or nonbinary, should be eating man-size portions to support that identity.

There is something beyond dystopian about the casual bringing up of hysterectomies (womb removal), oophorectomies (ovary removal), double mastectomies (breast removal) and phalloplasty (attachment of rolled up skin from the forearm or thigh to the groin) alongside haircuts and liking for sport, too. As though serious surgery is as superficial as the rest.
Numbers like (7) ‘menstruation status (whether you menstruate or not) and (8) ‘fertility status (whether fertile or not)’ are rather chilling. In the name of gender, doctors will take these natural, healthy bodily abilities from young women and girls and then have them take surveys to say they are “currently very satisfied” with the results of such cruelty.
Embodiment Goals
Embodiment goals might sound like something discussed, sorrowfully, at a Ghosts and Ghouls Anonymous meeting but it is used, in all seriousness, in this paper to apply to girls and boys who are already objectively embodied like the rest of us.
Here, the suggestion is that through the drugs on offer they will be able to achieve their “gender embodiment goals”. That jaunty little coinage feels, to me, like it might come with an unbearable hashtag as standard. One of the major challenges, apparently, is that when you give somebody cross sex hormones their body reacts, to some extent, in an individual way. So you can’t guarantee consumer satisfact…. I mean patient outcomes.
“Topical application of hormones to a specific organ still results in systemic absorption leading to systemic changes” which is, apparently, bad when you only want to affect one part of a whole human being, irrevocably.
The authors breezily admit that “there are no published protocols or data on body and mental health outcomes in persons who do not elect full hormone replacement” and that “many of these treatments lack high-quality evidence for use in gender-affirming care”. Despite that, and the fact they are paediatricians, this does not give them serious pause. Instead, they race to reassure the reader that “with an understanding of the physiology or the hormonal effects and pharmacology of the medications, tailored treatment regimens can be attained”.
This may, or may not, include “microdosing” which they mention. That is the practice of giving much smaller doses of cross sex hormones to individuals who call themselves nonbinary. On the basis, I suppose, that “sex is a spectrum” and, therefore, a dash of testosterone or a soupçon of oestrogen will take you to some other point on this mystical continuum.
Can I just remind everyone that these people are now talking about children and adolescents?
Essentially, what I am reading in this paper is that they have no evidence to justify what they are doing but they’re probably going to do it anyway. They neglect to mention, too, what risks there are for young people who go onto cross sex hormones.
In recent years, an increasing number of doctors in countries around the world have raised serious concerns about the use of puberty blockers in gender dysphoric children. This follows on from many years of women’s rights campaigners raising the alarm about the paucity of evidence, the potential harms and the regressive ideology being used to justify giving such powerful drugs.
Interestingly, this sea-change seems to have reached the doctors in Seattle. While others, in medicine, do argue for puberty suppression in young people claiming to be nonbinary the authors here acknowledge risks. They cite and discuss an article, on the subject, saying “ultimately, the authors agreed that long-term use of GnRHa was not a reasonable choice, and that the nonbinary individual could be supported with a number of other treatment options that could be individualized to their embodiment goals”
I am circumspect about the words “long term” there. Does that mean the short term usage of puberty blockers is considered OK by these doctors?
They certainly support the use of drugs such as spironolactone, finasteride, and bicalutamide for young male patients. While not strictly puberty blockers (GnRHas) they are still androgen blockers and therefore can have some effect on pubertal development. Spironolactone and bicalutamide, for example, have both been used in boys to help treat precocious puberty5 .
Finasteride, on the other hand, is not generally recommended for usage in children under 18 (or women)6 . So why are paediatricians mentioning its usage in a paper about their young patients at all?
The potential sides effects of these drugs can be serious, too. Potential impacts on the kidneys and liver, for example, would suggest these are not drugs to give off-label to children and adolescents on the basis of a ‘gender identity’.
Medicine really has yet to justify why, in this particular field, it is giving all manner of drastic interventions, to anyone, without a serious evidence base at all.
The discussion of androgen blocking drugs, by doctors at Seattle Children’s Hospital, does raise another question, as well. Now that puberty blockers are facing well-deserved scrutiny, are doctors simply going to turn to the nearest drugs that do similar work to give to children and adolescents? Is this the way they will evade criticism while doing essentially the same terrible thing as before?
I had this thought, and then spoke to a doctor friend of mine who raised exactly the same worry unprompted.
It certainly can’t be coincidence, either, that there is a repeating theme in other papers I dug up about the use of alternate drugs, in place of blockers. Several authors mention that these other drugs are covered by insurance where blockers were not. 7
The road to hell may be paved with good intentions but the road to gender affirmation is still paved with ready money.
SERMs
The paper soon goes on to suggest the possible use of SERMs (selective estrogen receptor modulators) in youths of both sexes who identify as nonbinary. These are drugs normally used by women for some types of breast cancer, and osteoporosis. Authors note that one of the side effect risks is an increased chance of deep vein thrombosis. They say this has only been evaluated in “cisgender women” as though the veins of a female with a different gender identity wouldn’t dare.
They then, again, have to point out that there is no solid evidence base here. Does it matter to them, really? Haven’t these children been essentially exempted from such ethical concerns?
There’s a bit of a contradiction of previous statements, too, as they specifically suggest SERMs might be useful for “nonbinary AFAB youth” who are already taking puberty blockers and don’t want to discontinue them. I thought we’d established that was a bad idea?
“For someone who has begun treatment with a GnRHa and does not desire to discontinue treatment or start testosterone, the addition of an SERM may be a temporary solution to provide estrogen agonist effects on bones without leading to breast development.”
I presume, from that context, that they think SERMs might help improve the bone density loss caused by the blockers but this seems, at least to a lay person like myself, like a total stab in the dark.
A basic Google of SERMs throws up these relevant pieces of information: that Raloxifene is the only SERM recommended for osteoporosis and, then, only for postmenopausal women. Unlike, say, “nonbinary youth” who are either male or barely past the age of menarche.
In fact, as well as an increased risk of uterine cancer for women, another serious and rare side effect of SERMs is thin bones in women who haven’t gone through the menopause yet.
So is the medical profession trying to turn the bones of these children into glass? Or is it the unintended consequence of this level of pseudoscience?
Non Medical Medicine
The paper ends with a detour into “nonhormonal options to affirm gender identity” which include hair and clothing, breast binding, packing, tucking genitalia, hair removal, and voice training.
Both the tucking of genitals for males, and binding of breasts for females, come with potential risks. From breathing difficulties, and even rib fractures, to testicular torsion and a potential reduction of viable sperm. But they’re affirming.
And affirmation is now being counted as far more important BY MEDICINE than the physical safety and health of youngsters.
“Legal gender affirmation, such as name change and gender marker change, can also be a way to affirm gender identity. The gender marker ‘X’ which may be most representative of nonbinary persons is available on US passports as of April 2022, in addition to driver’s licenses and birth certificates in many states.”
Is this a medical opinion, or merely an ideological one?
Lastly, the authors discuss surgery which, of course, is also “gender affirmation”. Before trans ideology came along I’m not sure anyone ever expected surgery to be affirming. Being cut open was largely a much more serious business before the invention of the pronoun circle.
“Some nonbinary persons may opt for surgical treatment with or without hormonal intervention” they tell us cheerfully. Adding “Gender-affirming surgeries are associated with improved mental health outcomes in gender-diverse adults, including nonbinary individuals.” I’m going to need to see the source on that8 .
The source on that, of course, does not justify offering surgeries to minors. Not least because it is not a study about minors. The limitations, too, are clear “ Non-probability sampling of the USTS may limit generalizability and Observational design may be vulnerable to unmeasured confounding.”
So it can’t be used to generalise but Seattle Children’s Hospital *can* use it to suggest surgical interventions on young people?
None of this is science. It’s like playing darts, with people’s lives, and just hoping to hit something resembling a positive outcome.
Final Thoughts
Western medicine is currently in thrall to trans ideology. It keeps insisting on the primacy of gender identity over biological sex and is willing to act accordingly even when the people in its care are young, impressionable and just beginning.
It appears, as yet, that there are little to no real brakes on this out of control clown car masquerading as healthcare. When one note of caution sounds, it just barrels along a different pathway. Even as more and more people question the medicalisation of children who claim to be the opposite sex, doctors are finding a way to medicalise those who claim to be neither.
The only way to make this stop is to refuse to be silent about it. When scientific enquiry falls to unreason, it’s on all of us to try and bring it back on course.
The “trans child” and the “nonbinary child” are not real. There is only the child.
She, or he, deserves infinitely better than all of this.
https://jme.bmj.com/content/46/11/743
https://journals.sagepub.com/doi/pdf/10.1177/20420188231160405
https://www.liebertpub.com/doi/10.1089/trgh.2020.0088
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8060208/#R24
https://pubmed.ncbi.nlm.nih.gov/8421081/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6431559/
https://www.nhs.uk/medicines/finasteride/#:~:text=3.-,Who%20can%20and%20cannot%20use%20finasteride,recommended%20for%20women%20or%20children.
https://www.thelancet.com/journals/landia/article/PIIS2213-8587(17)30099-2/fulltext
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6431559/
https://pubmed.ncbi.nlm.nih.gov/33909023/
good coverage
"What tangled webs we weave" when we first deceive ourselves, when we put feelings -- and economic self-aggrandizement -- ahead of facts and scientific principles. Though "codswallop" is probably being charitable -- "medical scandal" and "an egregious Big Lie" probably being more honest and accurate.
However, your “... 'Man is when short hair and rude in public' say progressives" underlines the dichotomy between sex and gender, between defining, for example, "woman" as "adult human female [AHF]" or as "anyone who has any sort of a passing family resemblance to AHFs".
More or less the dichotomy between monothetic categories and polythetic ones -- respectively. See this post of mine for some elaborations on the details in the context of defining sex as a binary or as a spectrum:
https://humanuseofhumanbeings.substack.com/p/binarists-vs-spectrumists
There is, in fact, some scientific, linguistic, philosophical, and logical justification for polythetic categories, for the concept of family resemblances. However, one of the major problems with them is that if one is not careful about who one lets into the family then one is likely to find oneself sitting down to Christmas dinner with the Manson family ... so to speak.